Even though prostate cancer progresses very slowly it is the second most deadly cancer for men in the united states therefore, the choice of treatment is very important. Moreover, a common antigen is expressed in almost every prostate cancer, prostate-specific membrane antigen (PSMA), which makes it the perfect therapeutic target.
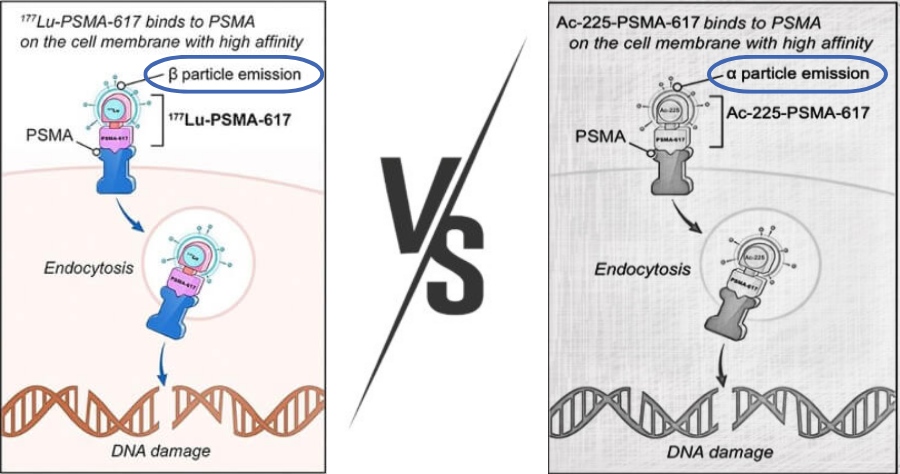
Different treatments are being used for metastatic castration-resistant prostate cancer (mCRPC) however the most promising are radioligand therapies, a radioactive compound that binds to the PSMA receptor present on the prostate cancer cell causing direct damage to the cancer cell by releasing a small amount of radiation.
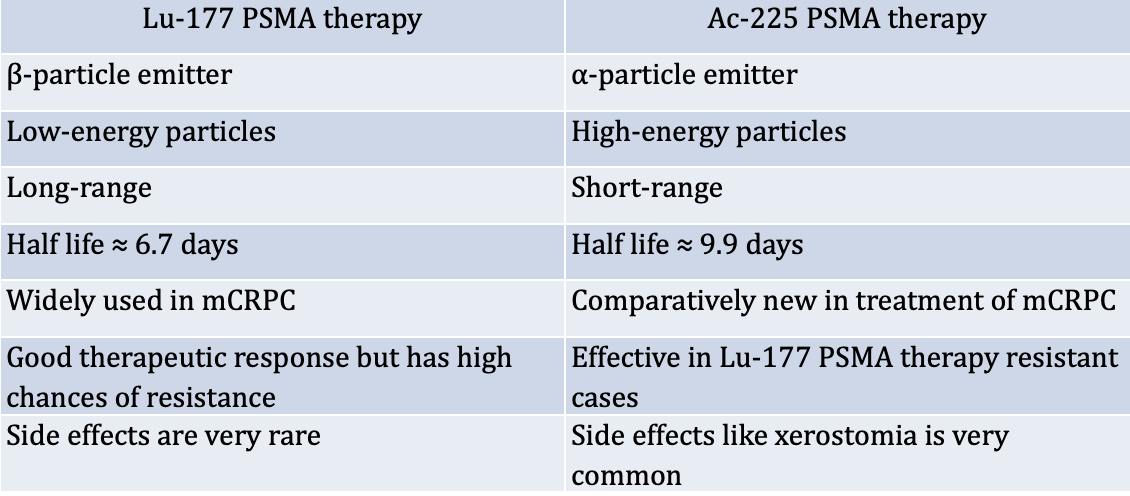
The most common radioligand therapies are Lu-177 PSMA therapy and Ac-225 PSMA therapy and the main difference is the type of radioactive compound. Lutetium-177 PSMA therapy uses a radioactive isotope of lutetium that damages DNA by emitting high-energy gamma rays. On the other hand, Actinium-225 PSMA therapy uses a monoclonal antibody radiolabeled with an isotope of actinium.
To know which therapy to take, different parameters should be taken into account that are discussed in this blog.
Which therapy to consider, Lu-177 PSMA or Ac-225 PSMA therapy?
Over the last few years, Lu-177 PSMA therapy has been commonly accepted in the treatment of metastatic castration-resistant prostate cancer patients (mCRPC) nevertheless, nearly 19.18% of patients are non-responders and show the progression of disease with an increase in prostate-specific antigen (PSA).
The question does arise on the effectiveness of Lu-177 PSMA therapy compared to Ac-225 PSMA. For which a comparative study was carried out on advanced metastatic castration-resistant prostate cancer patients where Ac-225 PSMA was administrated after failure on Lu-177 therapy and the results showed a considerable antitumor activity while using Ac-225 PSMA therapy. However, a major side effect which is dry mouth leads to stopping the therapy for a quarter of the patients.
Another study showed Ac-225 PSMA therapy as an efficacious salvage treatment option with low toxicities, which arises a new prospect for refractory or relapsed patients from conventional treatment as well as from Lu-177 therapy.
Difference between Lu-177 PSMA therapy and Actinium-225 PSMA therapy
Even though Ac-225 PSMA therapy is promising further studies are needed, and it is up to the doctor to decide which therapy to undertake.
Before Procedure comparison
The same pre-procedures are considered for both therapies which consist of:
- A recommendation of hydration: two to three glasses of water prior to arriving at the hospital
- Consumption of alcohol, aspirin, and anticoagulant are avoided
- A quality of life questionnaire will be given to be completed
- The doctor will take a routine baseline investigation, explain the procedure, answer questions, and will give a consent form to sign to authorize him to perform tests and give medicine.
- A 68-Ga PSMA PET CT scan is conducted before the therapy in case not performed earlier
During Procedure comparison
Before proceeding with the treatment, the temperature, pulse, and blood pressure will be taken.
Both treatments are administered intravenously and are administered over a period of 30 mins. After the administration, the patient is kept under observation for about 24-48 hours.
If needed, medications to relieve the symptoms are provided by the doctor.
Post Procedure comparison
The temperature, pulse, and blood pressure will be taken again.
Radiation levels are checked and as soon as they reach a safe level the patient can be authorized to leave. Patients who undertook Lu-177 PSMA therapy can leave after two hours but they are usually kept under a doctor’s supervision for 2-3 days same as in the case of Ac-225 radiotherapy patients and are allowed to leave after full body scintigraphy is performed to estimate the absorbed doses of radioligand by the organs and tumor lesions.
Nevertheless, the following precautions should be taken into account by the patient, until advised otherwise by the doctor:
- Staying hydrated is primordial
- Lifting heavy things should be avoided
- Serious activities 24 hours post-therapy are avoided
- Sexual activity is avoided
- Unusual bleeding or bruising should be informed instantly
Follow up comparison
Follow-up appointments consist of physical checkups and laboratory examinations, different information on tests and checkups will be given in a written statement, other supplementary medications can also be suggested and any question should be addressed to the doctor.
Lutetium therapy follow-up depends on each patient. Some patients only need a single treatment while others may need multiple treatment cycles which can range from 2-6 cycles with a 6-8 weeks gap between each one of them.
Actinium therapy follow-up depends on the spread of cancer during initiation of the therapy and the response of the therapy. The patients usually receive few cycles however, late-stage prostate cancers that are widely spread may require more cycles.
The decision on the treatment plan should be made with the doctor as he is aware of the different suitable substitute approaches as well as recovery time, side effects, and costs.
Side Effects comparison
Side effects can take place because of the presence of radiation in the body
Following are typical side effects of Lutetium 177 PSMA Therapy:
The most common side effects include:
- Dry Mouth
- High bleeding risk
- Fatigue
- Nausea
Rare side effects include:
- Headache
- Fever
- Skin rash
- Bone marrow suppression
- Low blood counts
Following are typical side effects of Actinium-225 PSMA therapy
The most common side effects include:
- Dry mouth (most common)
- Anemia (low red blood cell count).
Rare side effects include:
- Decrease in iron, calcium, magnesium, phosphate, or vitamin B12 levels
- Short-term bone density loss as well as minor decrease of bone mineral density but fortunately go back to normal within six months.
Additional very rare complications due to radiation exposure during radioligand PSMA therapy may include:
- Kidney Problems
- Cardiovascular Disease (heart disease)
- Nerve Damage
- Radiation Myelopathy (paralysis condition due to nerve damage)
- Sexual Dysfunction
The doctor should be informed about any other side effects to avoid further complications.
Prognosis comparison
Radioisotope therapy responders with advanced metastatic castration-resistant prostate cancer show an average progression time of 12.5 months and overall survival of 32.6 months while the nonresponders show an average progression time of 1.4 months and overall survival of 7.3 months
Lutetium177 PSMA therapy is successful for almost 80% of prostate cancers still, some patients require additional treatment cycles. On the other hand, a study showed that Actinium 225 PSMA therapy improved the survival rate in cases where Lu-177 PSMA therapy failed and decreased treatment-related toxicity.
225Ac-PSMA and 177Lu-PSMA combined therapy of metastatic castration-resistant prostate cancer is also currently under trial.
Compared to conventional drug treatment, the cost of radioligand treatment is higher due to the complexity of synthesis. However, the total expenses are lower because of the non-requirement of unnecessary additional drugs since the treatment is well tolerated by patients.
The cost for the treatment of advanced metastatic castration-resistant prostate cancer differs between different hospitals. Lutetium therapy cost ranges from 7,500 € to 16,000 € in specialized hospitals covering all steps of the procedure including the follow-up. On the other hand Actinium therapy cost ranges from 8,000 € to 17,000 € for each cycle.

Comments